Patients with acute RVO most commonly present with painless, blurred vision, vision loss, or floaters.1 The initial exam should include visual acuity, pupillary assessment, slit-lamp exam looking for new iris vessels, measurement of intraocular pressure, binocular funduscopic evaluation of posterior pole, and gonioscopy for evaluation of iridocorneal angle.2 Dilated fundus exam may reveal intraretinal hemorrhages, dilated and tortuous retinal veins, retinal edema, exudates, and cotton wool spots.3 As patients with RVO may also have elevated ocular perfusion pressure or arteriovenous nicking with focal narrowing, optic nerve head (ONH) evaluation is necessary for all patients with RVO to rule out glaucoma.3 Color and red-free fundus photography are useful to document the severity of the retina findings.3,4 Artificial intelligence is being evaluated as an adjunct to clinical practice, with deep learning algorithms demonstrating good performance in recognizing RVO from color fundus photographs.2
Optical Coherence Tomography (OCT) is used to determine retinal thickness and to monitor macular edema and vitreoretinal interface changes.2 Treatment decisions are commonly based on OCT measurements because they are objective and quantifiable.2 Visualization of microvasculature of the retina and choroid is possible utilizing Optical Coherence Tomography Angiography (OCTA), a non-invasive way to detect capillary nonperfusion, enlarged avascular zones, and vascular abnormalities.2 Fluorescein angiography is useful in assessing retinal ischemia, delayed vein filling, the presence of retinal neovascularization with fluorescein leakage, and collateral vessels.3,4
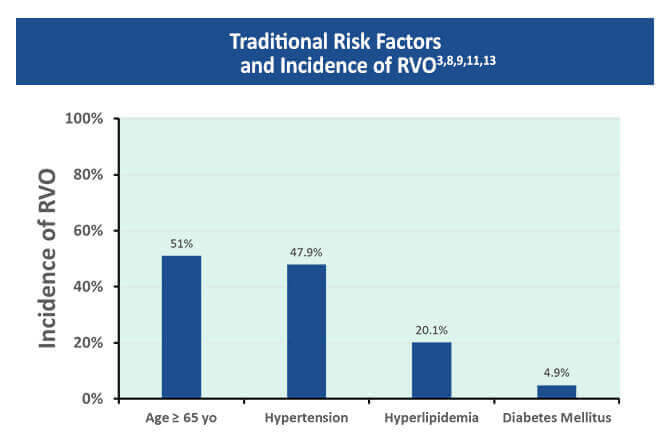
Clinicians need to educate their patients about risk factors that increase their chances of developing an RVO. Linkage of RVO to certain systemic vascular risks including hypertension, hyperlipidemia, diabetes, active smoking, and peripheral vascular disease has been made.3,5-7 A meta-analysis found that 47.9% of RVO cases were attributed to hypertension, 20.1% to hyperlipidemia, and 4.9% to diabetes.2,3,8 Hypertension can cause a thickening or hardening of the overlying artery, which causes turbulent blood flow that is believed to promote venous thrombosis.9 The occlusion can obstruct blood flow and increase venous pressure.2,10 This may lead to vascular leakage and edema, hemorrhages, and ischemia.9
Fifty-eight percent of patients with CRVO onset at an age younger than 50 years were found to have a nontraditional risk factors, such as an underlying systemic disease, hypercoagulability, or history of hormonal contraceptives on evaluation.11 In a cohort with systemic lupus erythematosus, the incidence of CRVO was 3.5 times higher than in a control population.10,11 Although men and women are affected equally, the incidence of RVO increases with age, with >50 % of cases occurring in patients over 65 years old.9
Systemic factors that protect against BRVO include increased high density lipoprotein (HDL) levels, moderate alcohol consumption, and increased exercise.3 In contrast, only increased physical activity has been shown to protect against CRVO.3,6 Communication with the primary care provider is essential, since patients with RVO may have a higher risk of cardiovascular disease and cerebrovascular accidents.3,12